- What is pneumothorax?
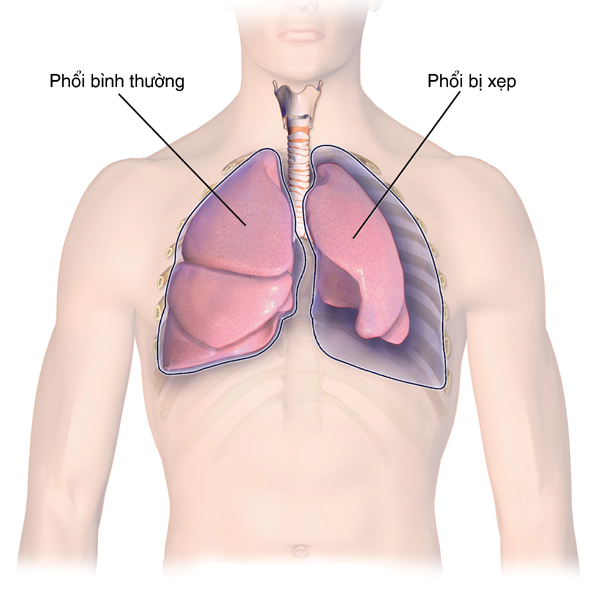
A pneumothorax is a condition where air leaks through a hole in the lung, causing air to fill the pleural cavity. As the amount of leaking air increases, the lung cannot function normally. If the air in the chest cavity is not removed, the space between the lung and heart can be pushed to the opposite side, leading to a medical emergency.
- Causes of pneumothorax
- Symptoms of pneumothorax
- Diagnosis of pneumothorax
The easiest way to diagnose pneumothorax is through a chest X-ray. A chest X-ray, combined with the symptoms mentioned above, can be used to diagnose pneumothorax in most cases. Additionally, diagnosis can be based on other test results from the patient. Pneumothorax may be suspected by tapping the affected area, performing a spectral magnetic resonance, and noting decreased breath sounds during auscultation. A chest X-ray will be performed and the results will be interpreted by a specialist to confirm pneumothorax.
In recent years, high-resolution computed tomography (HRCT) of the lungs has been utilized to diagnose and establish treatment methods. The aim is to determine whether the patient with pneumothorax requires surgical intervention. However, this test is not necessary for all patients, so it is advisable to consult a specialist to determine what examinations are needed.
- Treatment of pneumothorax
The principle of treating pneumothorax is to remove the leaking air from the lungs in the chest cavity to allow for lung re-expansion, and to effectively seal the chest cavity to prevent recurrence. Treatment for pneumothorax is determined based on the patient’s condition and whether there is a recurrence. The duration of treatment for pneumothorax is difficult to predict. Most patients require treatment for about a week. Some patients may need treatment for a longer duration, even in cases of spontaneous pneumothorax. Generally, the treatment duration for secondary pneumothorax is significantly longer than for spontaneous pneumothorax, and it is challenging to choose the appropriate treatment method, so it is advisable to follow the guidance of a specialist.
- Monitor & note for pneumothorax
If a pneumothorax is initially treated with observation or simple chest tube placement, the recurrence rate is about 50%. If it has recurred twice, the risk of recurrence more than three times is approximately 80-90%. Therefore, patients with recurrent pneumothorax need to be treated surgically. The recurrence rate in patients who have undergone surgical treatment is about 5%.
In high-altitude areas, the air pockets in the lungs can easily rupture. Those who have been diagnosed with pneumothorax or who are at risk of recurrence should consult a specialist before undertaking long trips.
Deep inhalation of smoke and heavy breathing after strenuous exercise can increase chest pressure along with abdominal pressure. This pressure can easily rupture bubble-like pockets in the thin pleura, so caution is advised.